
Diagnosing AADC
deficiency
AADC deficiency may be misdiagnosed or go undiagnosed, delaying treatment and proper management 3,4,12
Despite symptom onset during infancy, diagnosis is typically delayed 3:
Mean age of symptom onset
2.7 months
Mean age of diagnosis
3.5 years
Age range of diagnosis
2 months to 23 years
Symptoms of neurotransmitter disorders can overlap with those of other neurological disorders, which can make diagnosis challenging. Many of the most common symptoms of AADC deficiency can also be attributed to a number of other conditions such as cerebral palsy and epilepsy, resulting in potential misdiagnosis.1-4,7-9
The challenge of a correct diagnosis:
conditions with symptoms similar to those of AADC deficiency
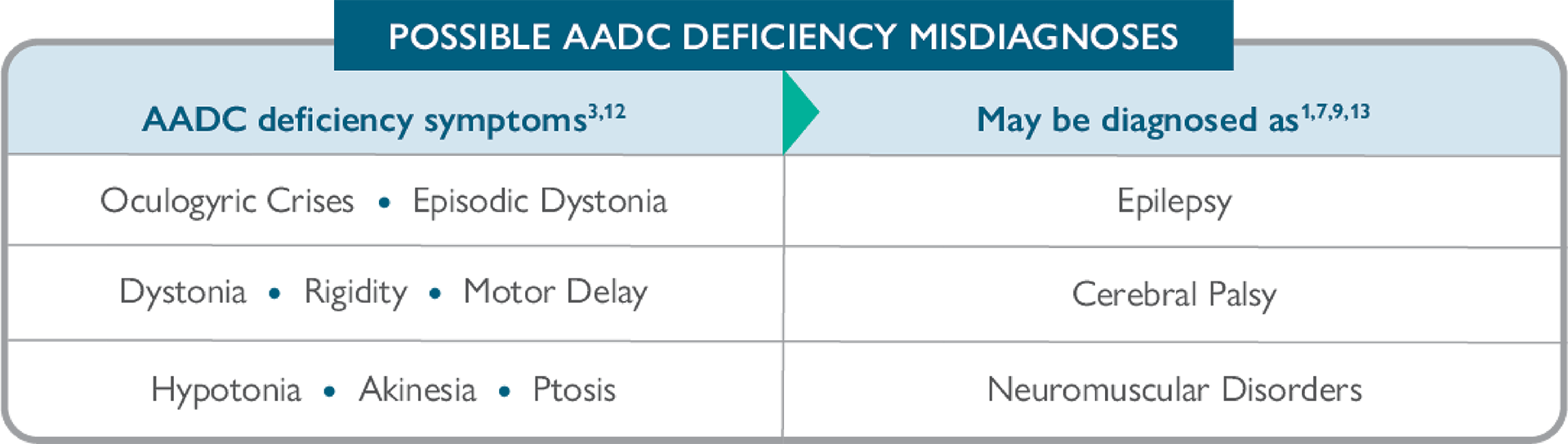
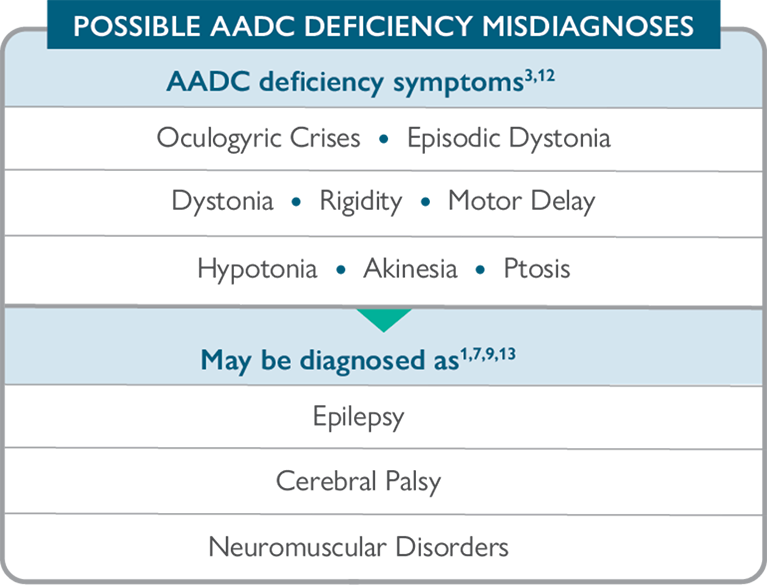

If you have patients with cerebral palsy of unknown aetiology or patients with epilepsy that is refractory to treatment, you may want to consider an alternate diagnosis of a neurotransmitter disorder such as AADC deficiency.
Look for key differentiating signs and symptoms of AADC deficiency
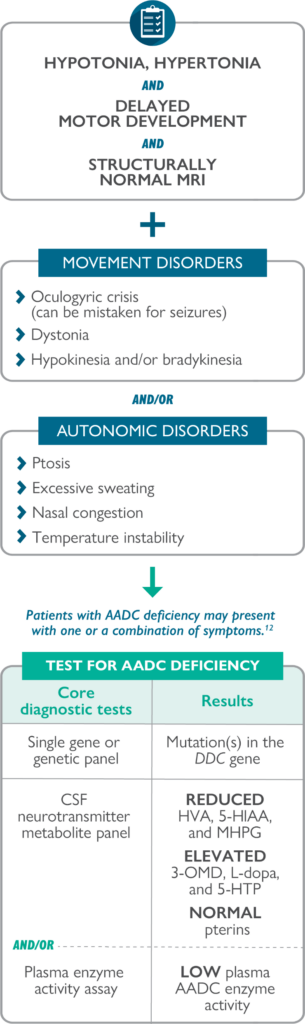
One or a combination of the following red-flag diagnostic clues should prompt investigation for a neurotransmitter disorder, including AADC deficiency:

Oculogyric crises4,12,14
Episodes of sustained upward or lateral deviation of the eyes, rhythmic orofacial movements, backward and lateral flexions of the neck, tongue protrusion, and jaw spasms that can sometimes be confused with seizures8,11
Normal EEG and neuroimaging3,7,8,12
One study showed that only a small proportion of patients with AADC deficiency had an abnormal EEG, MRI, or CT4

Autonomic symptoms12
Multiple signs of autonomic dysfunction8

Diurnal variation1,3,15
Motor symptoms become exacerbated or more prominent late in the day and improve with sleep1,15
CT=computer tomography; EEG=electroencephalogram; MRI=magnetic resonance imaging.
Accurate identification can help improve the care and management of patients with AADC deficiency10,12
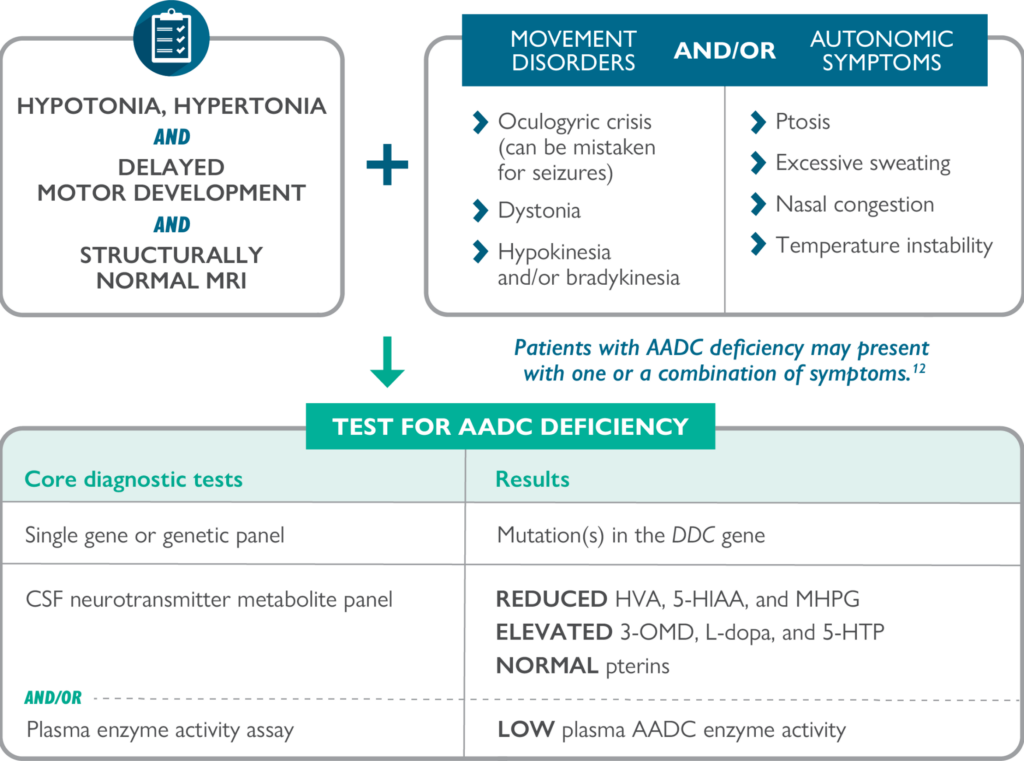
Diagnostic pathway for suspected AADC deficiency 3,12
Other tests that may be helpful include16-19:
Blood level measurement of 3-OMD
Urinary organic acid analysis

Current consensus guidelines recommend performing a CSF neurotransmitter metabolite panel and/or plasma AADC enzyme activity assay in combination with genetic testing to confirm a diagnosis of AADC deficiency. 3

Download a Diagnosis Guide to help confirm AADC deficiency
Why test for 3-OMD?
Reduced AADC enzyme activity causes an increase in L-dopa, 3-OMD, and 5-HTP, and a decrease in the neurotransmitter metabolites HVA and 5-HIAA.3,4,10,11

Typically, the diagnosis of AADC deficiency requires CSF neurotransmitter analysis. However, 3-OMD, which is a catabolic product of L-dopa that accumulates in individuals with AADC deficiency, can be detected in their blood. 3-OMD measurement in plasma represents a less invasive, simple, rapid, and valid measure for detecting AADC deficiency. 17,19
References
1. Ng J, Papandreou A, Heales SJ, et al. Monoamine neurotransmitter disorders—clinical advances and future perspectives. Nat Rev Neurol. 2015;11(10):567-584. 2. Ng J, Heales SJR, Kurian MA. Clinical features and pharmacotherapy of childhood monoamine neurotransmitter disorders. Pediatr Drugs. 2014;16(4):275-291. doi: 10.1007/s40272-014-0079-z. 3. Wassenberg T, Molero-Luis M, Jeltsch K, et al. Consensus guideline for the diagnosis and treatment of aromatic l-amino acid decarboxylase (AADC) deficiency. Orphanet J Rare Dis. 2017;12(1):12. doi: 10.1186/s13023-016-0522-z. 4. Brun L, Ngu LH, Keng WT, et al. Clinical and biochemical features of aromatic L-amino acid decarboxylase deficiency. Neurology. 2010;75(1):64-71. 5. Manegold C, Hoffmann GF, Degen I, et al. Aromatic L-amino acid decarboxylase deficiency: clinical features, drug therapy and follow-up. J Inherit Metab Dis. 2009;32(3):371-380. 6. Hwu W-L, Chien Y-H, Lee N-C, et al. Natural history of aromatic L-amino acid decarboxylase deficiency in Taiwan. JIMD Rep. 2018;40:1-6. doi: 10.1007/8904_2017_54. 7. Kurian MA, Dale RC. Movement disorders presenting in childhood. Continuum (Minneap Minn). 2016;22(4):1158-1185. 8. Zouvelou V, Yubero D, Apostolakopoulou L, et al. The genetic etiology in cerebral palsy mimics: the results from a Greek tertiary care center. Eur J Paediatr Neurol. 2019;23(3):427-437. doi: 10.1016/j.ejpn.2019.02.001. 9. Krigger KW. Cerebral palsy: an overview. Am Fam Physician. 2006;73(1):91-100. 10. Pons R, Ford B, Chiriboga CA, et al. Aromatic L-amino acid decarboxylase deficiency: clinical features, treatment, and prognosis. Neurology. 2004;62(7):1058-1065. 11. Hwu W-L, Lee N-C, Chien Y-H, et al. AADC deficiency: occurring in humans, modeled in rodents. Adv Pharmacol. 2013;68:273-284. 12. Himmelreich N, Montioli R, Bertoldi M, et al. Aromatic amino acid decarboxylase deficiency: molecular and metabolic basis and therapeutic outlook. Mol Genet Metab. 2019;127(1):12-22. doi: 10.1016/j.ymgme.2019.03.009. 13. Lee W-T. Disorders of monoamine metabolism: inherited disorders frequently misdiagnosed as epilepsy. Epilepsy Seizure. 2010;3(1):147-153. doi: 10.3805/eands.3.147. 14. Pearson TS, Gilbert L, Opladen T, et al. AADC deficiency from infancy to adulthood: symptoms and developmental outcome in an international cohort of 63 patients. J Inherit Metab Dis. 2020;43(5):1121-1130. doi: 10.1002/jimd.12247. 15. Pearson TS, Pons R, Ghaoui R, et al. Genetic mimics of cerebral palsy. Mov Disord. 2019;34(5):625-636. 16. Monteleone B, Hyland K. Case report: discovery of 2 gene variants for aromatic L-amino acid decarboxylase deficiency in 2 African American siblings. BMC Neurol. 2020;20(1):12. doi: 10.1186/s12883-019-1596-8. 17. Chen P-W, Lee N-C, Chien Y-H, et al. Diagnosis of aromatic L-amino acid decarboxylase deficiency by measuring 3-Omethyldopa concentrations in dried blood spots. Clin Chim Acta. 2014;431:19-22. 18. Chien Y-H, Chen P-W, Lee, N-C, et al. 3-O-methyldopa levels in newborns: result of newborn screening for aromatic L-amino-acid decarboxylase deficiency. Mol Genet Metab. 2016;118(4):259-263. doi: 10.1016/j.ymgme.2016.05.011. 19. Brennenstuhl H, Kohlmüller D, Gramer G, et al. High throughput newborn screening for aromatic L-amino-acid decarboxylase deficiency by analysis of concentrations of 3-O-methyldopa from dried blood spots. J Inherit Metab Dis. 2020;43(3):602-610. doi: 10.1002/jimd.12208.